

Ultrasound imaging is widely accepted as an incredibly powerful tool for MSK and it is often the primary diagnostic tool in many musculoskeletal injuries. As ultrasound systems have become increasingly portable and more affordable, they are being used by clinicians across diverse medical specialties.
That’s why we weren’t surprised to see more than 2000 MSK clinicians registered for a recent webinar co-hosted by Clarius and Sonoskills — Pragmatic MSK Ultrasound: Scanning the Rotator Interval, Common Extensor Tendon and Patellar Tendon.
Presented by renowned ultrasound educator, Marc Schmitz, the webinar covered practical scanning skills to help make a confident diagnosis and expedite the right treatment plan for rapid recovery. Watch the one-hour webinar now or read on for some highlights on how to use ultrasound to diagnose and rule out rotator interval injuries.
Rotator Interval (Sono) Anatomy
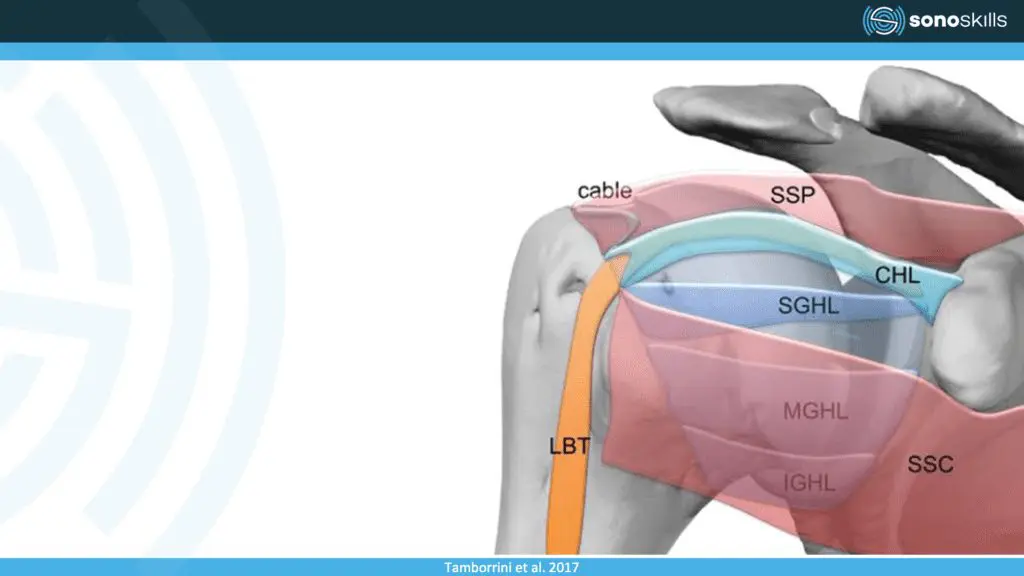
Let’s start by reviewing the sonoanatomy of the rotator interval. It is situated in the superior anterior shoulder in between the supraspinatus and the subscapularis. This is a zone where there is no rotator cuff and we find three structures: the long head of the biceps tendon, the coracohumeral ligament and the superior glenohumeral ligament. I like to bring attention to this structure as this is a region which is not included in most standard exams. I have adopted it as a standard practice as it brings me a lot of information.
Possible pathologies: signs of tendinosis of the biceps, biceps instability, a frozen shoulder or problems with ligaments.
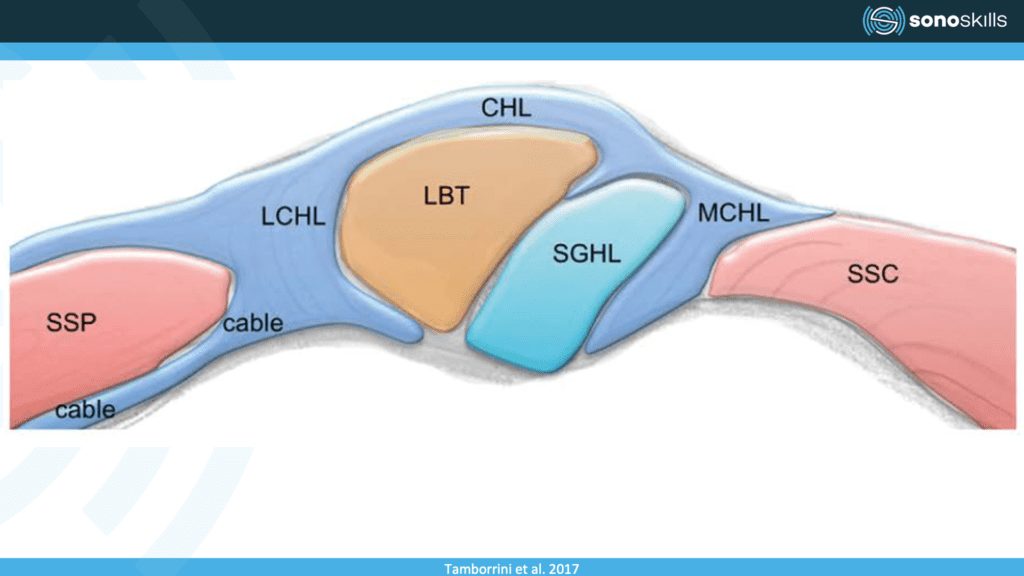
This image is a cross section of the rotator interval and here on the left side, you see the lateral side, the supraspinatus tendon, and on the right, we can see the subscapularis. And in between in the middle, we can see the long head of the bicep standard. This long head of the biceps is stabilized by this coracohumeral ligament, which is wrapping like an envelope around the tendon and is a small but important structure. Right next to the biceps tendon on the medial side of the long head of the biceps, we can also find the superior glenohumeral ligament. It often pays off to check this structure as it is typically more involved than people think.
Where to Scan for the Rotator Interval
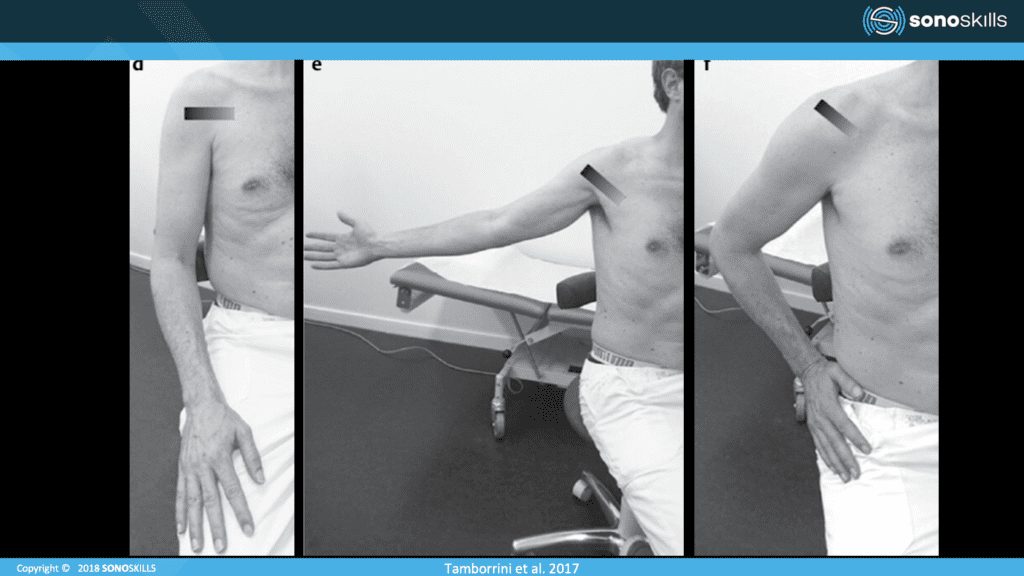
VIDEO: How to Scan the Rotator Interval
Watch this 3-minute video demonstration of March Schmitz scanning the rotator interval. He scans using the posterior approach, which is common in England, Sweden and the Netherlands. The ventral approach, or the Mediterranean way, is seen in Spain and Italy.
A Look at Various Sonopathology and Possible Diagnoses
In this image, you see the long head of the biceps, and we can see that the bicep actually looks okay. The bicep doesn’t seem to be tendinopathic, it’s not enlarged. There are no really dark zones, hypoechoic zones within the tendon.
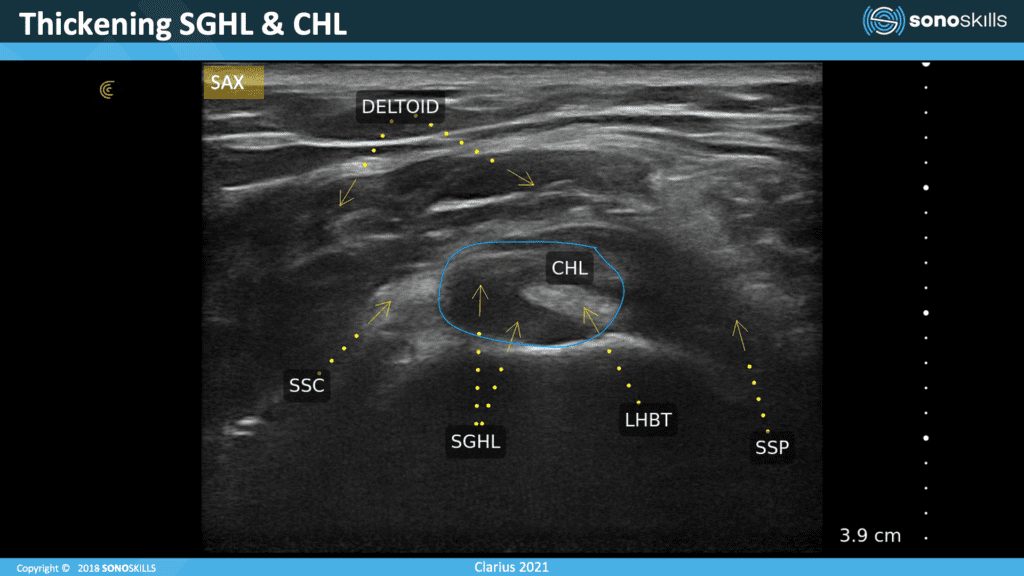
You can see the problem on this side. This superior glenohumeral ligament looks enlarged meaning that the capsule is irritated. At this point, I would switch on Doppler l to see whether there is inflammation here – to see if we can find neovascularization.
The coracohumeral ligaments also looks a little bit thickened. It’s hard to quantify the dimensions of the superior humeral ligament. Use also the other shoulder to compare in the left, right comparisons.
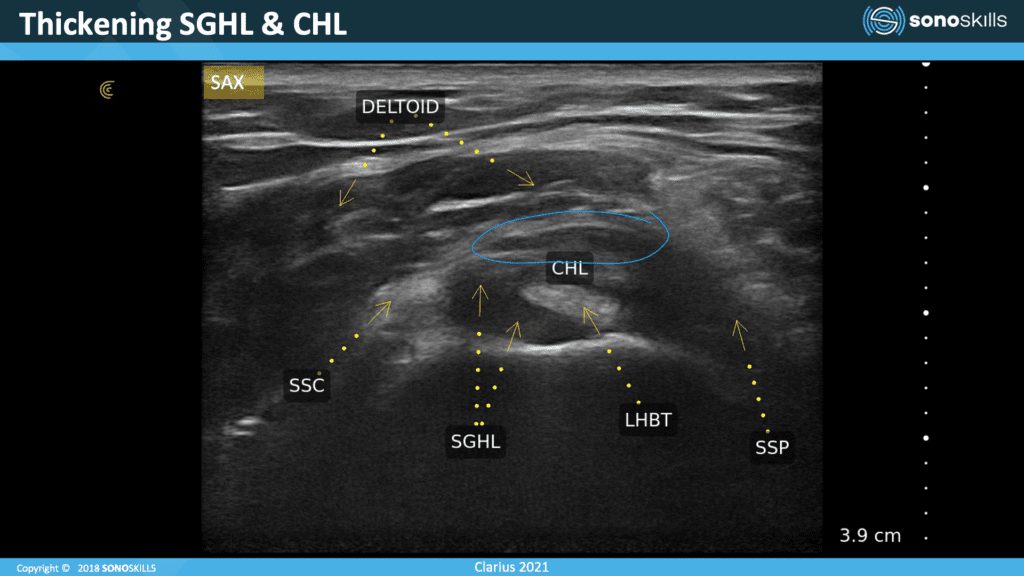
Here we can see a bursa effusion in the superchromial subdelta bursa. In the video we saw that it was only a hypoechoic thin line, but here we can see this effusion. So, we see thickening of the ligaments and also a swelling of the bursa.
Pathology: Increase of the Coracohumeral Ligament
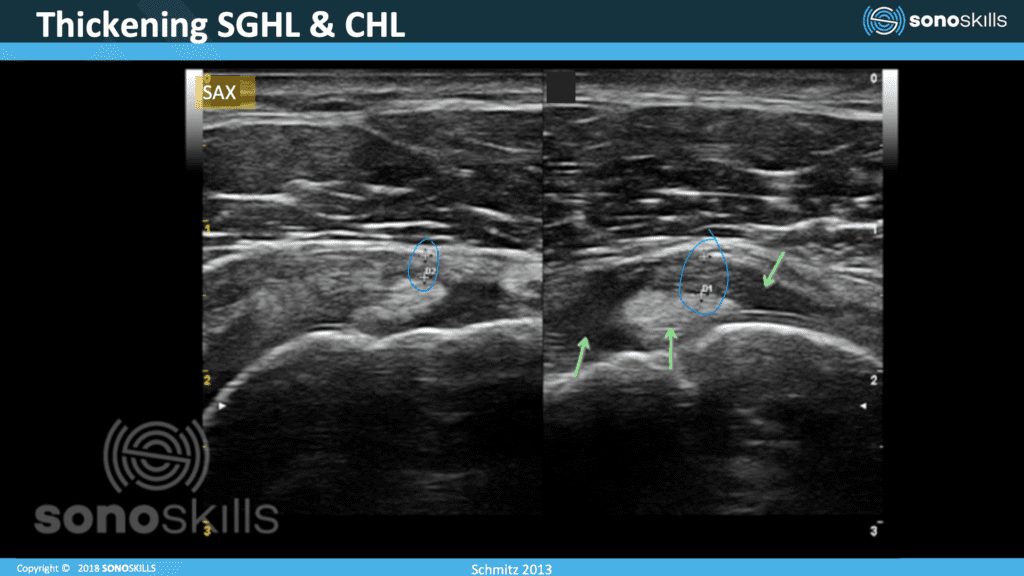
This image shows you the increase of the coracohumeral ligament. Sometimes the superior of the coracohumeral ligament can thicken significantly. This is a sign of capsulitis or frozen shoulders.
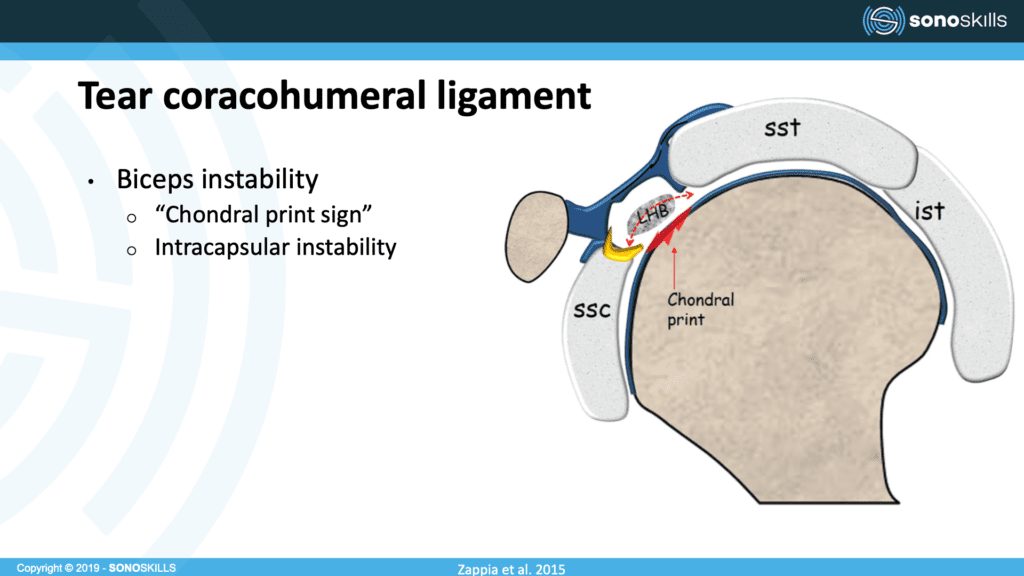
Besides looking for thickening of the ligaments and swelling of the bursa, check the long head of the bicep to see if it’s tendinopathic or torn. If it’s a full tear of the biceps, also check the rotator interval to see if the biceps is truly absent because you need to differentiate between anisotropy and a full thickness tear. Could the biceps be lopsided to medial? When you go to the rotate interval and you find a biceps tear, then it’s probably anisotropy. If you cannot find it in a rotator interval, it has to be pathology.
If there is an instability of the long head of the biceps, there might be some shearing forces between the bone and the biceps tendon, and then chondral print sign might happen, which is irregularity of the humeral head due to these shearing and frictional forces.
Pathology: Tear Subscapularis
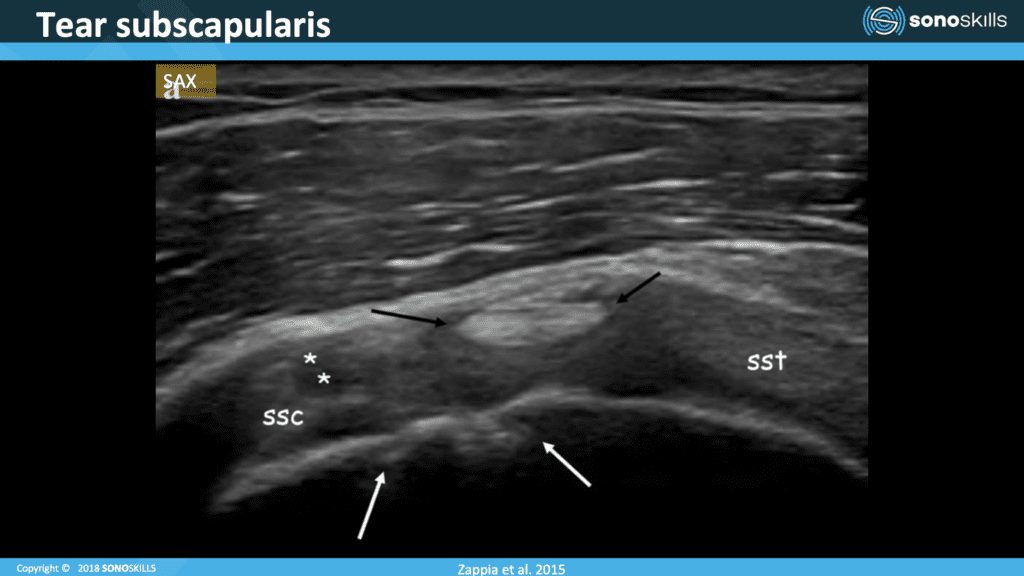
In this image, we can see that the biceps is quite high in the rotate interval. Usually it has an oblique position, one tip close to the bone. The other side is a little bit on top of the superior glenohumeral ligament, but in this case, we can see the biceps is high. There is a tearing of the coracohumeral ligament. We can see chondral print sign, a sign of instability and we can also observe that this part of the subscapularis has been torn.
The Role of Ultrasound in Diagnosing Adhesive Capsulitis/Frozen Shoulder
The European Society of Musculoskeletal Radiology has made consensus statements about use of ultrasound as the preferred imaging technique for a number of pathologies. They are currently slightly in favor of using ultrasound. But the clinical picture is still more important with patients suffering from frozen shoulder. The most important clinical cure is still passive external rotation limitations.
Still, my advice is to use ultrasound to consider the following indications:
- Thickening coracohumeral ligament
- Rotator interval: hypoechoic and increased power Doppler
- Exclude massive rotator cuff tear
- Coracohumeral ligament near coracoid process
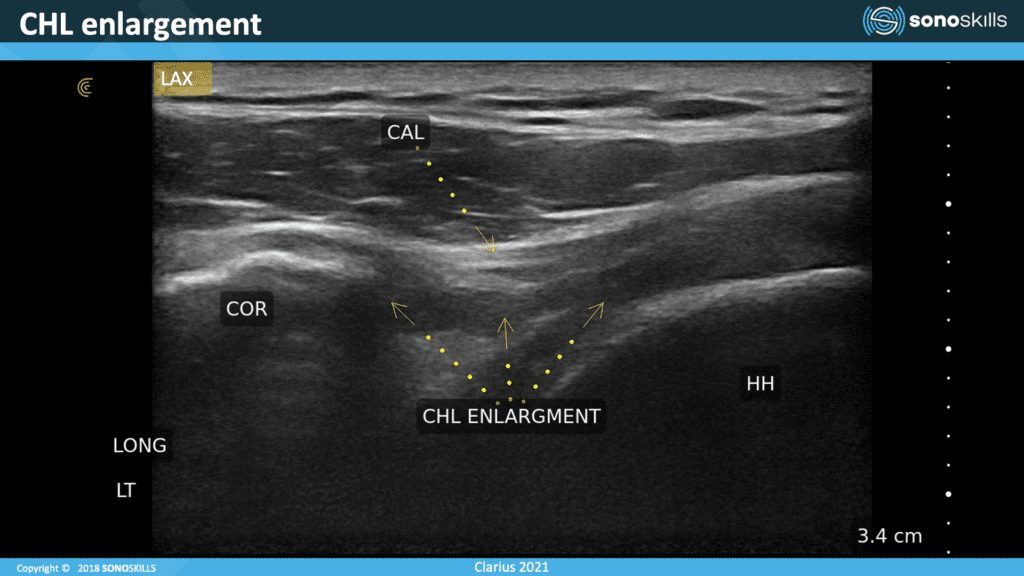
In this image, you see what the coracohumeral ligament enlargement looks like. It can thicken near the coracoid process, so not only near the biceps, but also near the coracoid process.
Note the coracoid process (COR), and the coracoacromial ligaments (CAL), and this is the coracohumeral ligament (CHL). We can see a thickening of this ligament, usually it’s thin and quite hyperechoic and some people even think that this is the acromial ligament, but it’s truly a different ligament.
Ultrasound Guidance Is Recommended for Frozen Shoulder Injection
While ultrasound is secondary to the clinical picture in diagnosing frozen shoulder, using ultrasound guidance to inject a frozen shoulder can help accelerate treatment. Landmark-based injections are not as effective or patient friendly. There is clear evidence that ultrasound-guided intervention is less painful for the patient. The patient can also see that the needle is where it should be and as a result the patient is more likely to trust the therapy. I definitely recommend using ultrasound to for injections.
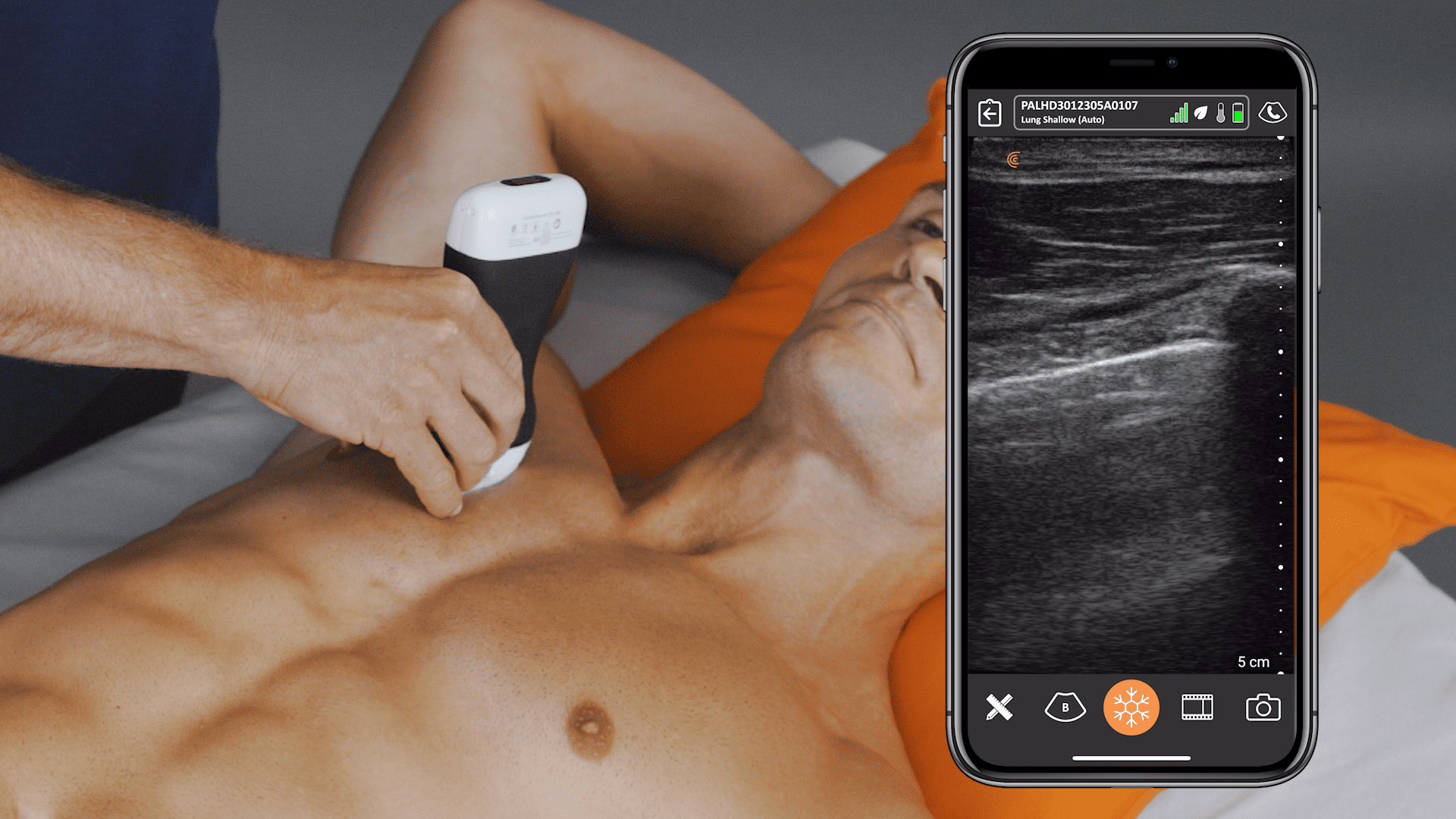
Handheld Ultrasound Designed for MSK Clinicians
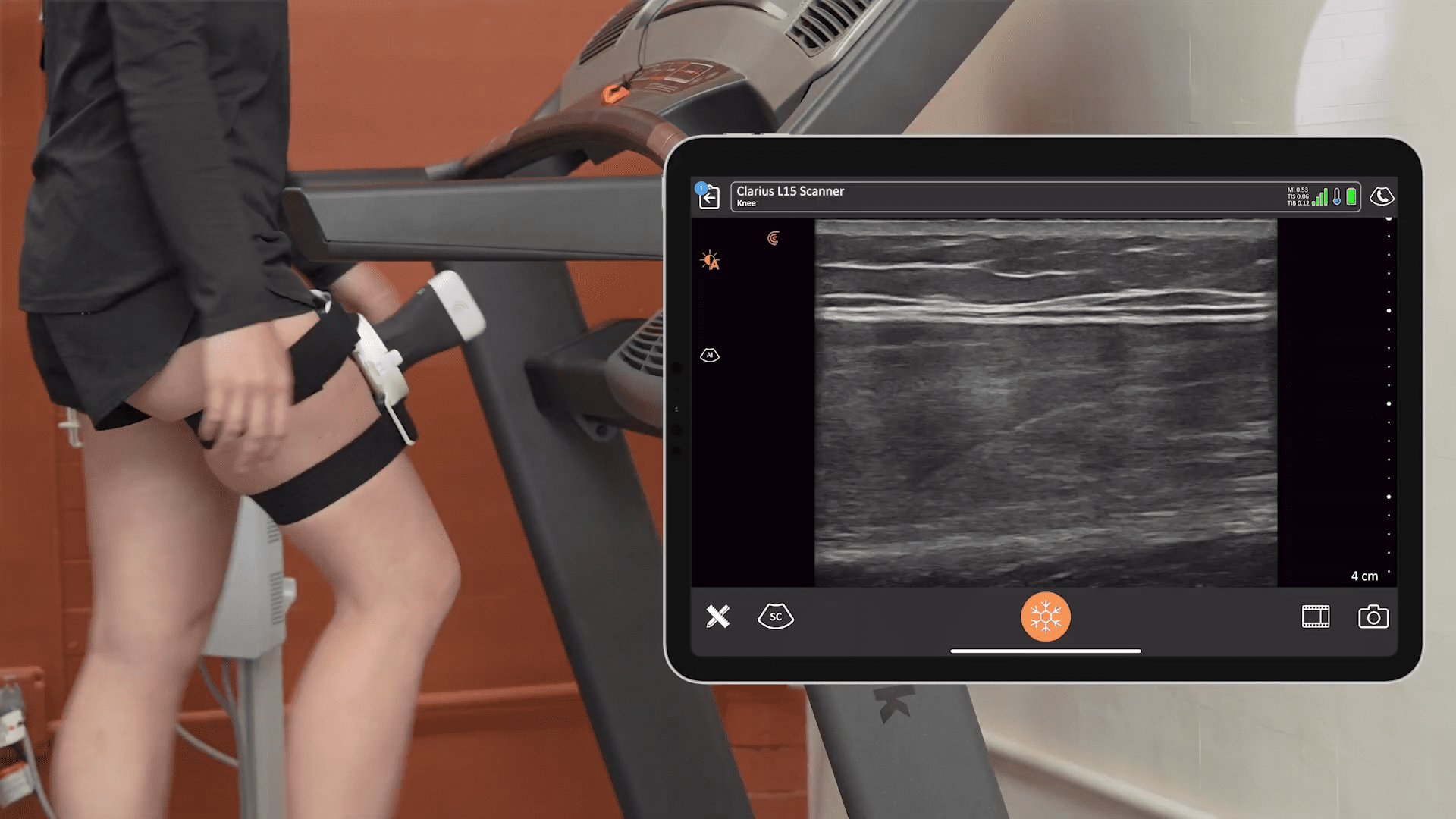
Getting detailed ultrasound images of musculoskeletal anatomy to make a confident diagnosis has never been easier. Ideal for MSK anatomy down to 7 cm, the Clarius L15 HD high-frequency ultrasound scanner is available with an optional Advanced MSK Package for diagnostic and interventional procedures.
Clarius offers four ultrasound scanners that are suitable for MSK applications. Learn more about which Clarius Handheld Ultrasound scanner is right for your practice. Or contact us today to request an ultrasound demo.










{kind=link}