In a recent webinar, Dr. Greg Hickman, Medical Director and Anesthesia Director at the Andrews Institute Ambulatory Surgery Center in Florida, shared his ultrasound-guided nerve block techniques for more effective regional blocks in patients undergoing knee surgery. Read the blog for highlights of Dr. Hickman’s technique for the ultrasound-guided adductor canal continuous catheter placement
Dr. Hickman has perfected his block techniques over the past 30 years and enjoys sharing what he’s learned during webinars like these and through his popular regional guided anesthesia educational website Blockjocks.com. He sees ultrasound as a huge advantage.
It improves your speed of being able to do the block, and it actually improves the duration of the block because you’re getting more local around the target nerve versus doing it blind where you really don’t see it. It should help anyone’s confidence in what they’re doing to be able to see what they’re doing.”
How and Where to Place an Adductor Canal Continuous Catheter Optimal Post-Op Pain Control
Adductor canal catheters are often placed at the mid-thigh level, but with knee surgeries performed at the Andrew’s Institute, Dr. Hickman and his team noticed a significant amount of their patients developed significant saphenous neuropathies – numbness from the knee to the ankle, and on occasion, some patients would even get a burning pain from this saphenous nerve. The solution was to place the adductor canal more proximally, toward the femoral triangle.
It was really important to me not to have pro football players playing with a little numbness on the inside of their lower leg from the knee to the ankle. And actually, the other thing I noticed, we got a little bit better analgesia.”
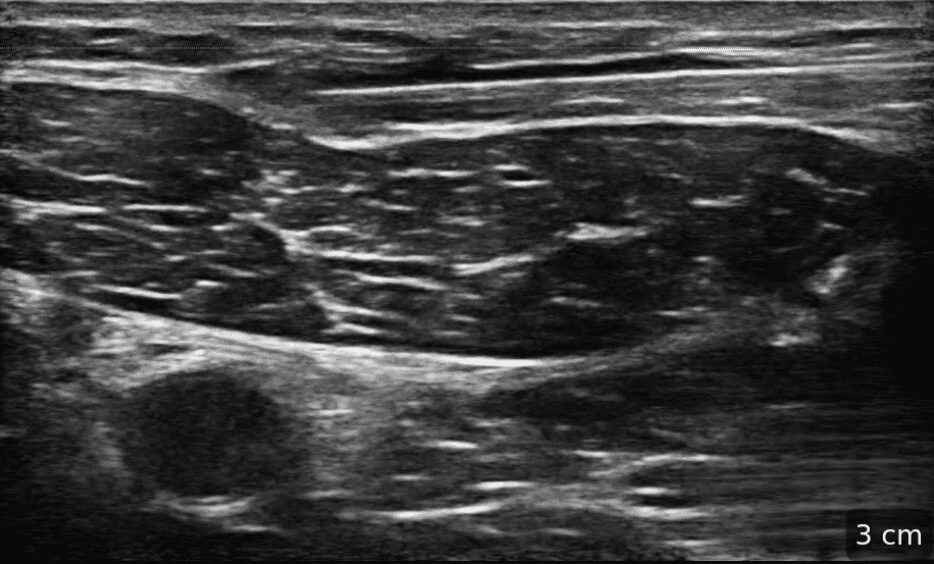
To locate the precise level for the catheter in the proximal adductor canal, Dr. Hickman uses high-resolution ultrasound to scan in the transverse plane, to locate the sartorius muscle and the femoral artery just deep to it. If you visualize the femoral artery centrally behind the sartorius, you’re too far down the adductor canal.
This image demonstrates the level of the saphenous verve and the verve to the vastus – we know they’re closer together here, and will result in better anesthetic

In under 5 minutes, Dr. Hickman demonstrates his ultrasound technique to locate the best spot in the proximal adductor canal to guide the catheter to. With increased accuracy, he only needs to inject 10 – 15 cc’s, which will ensure the femoral nerve isn’t blocked.
Something New for Post ACL Repair Pain Control
Pain management following ACL repair has come a long way since the early 1990’s. Gone are the days when patients spent 3 days in the hospital, to the present day when the surgery is done on an out-patient basis.
Innovators like Dr. Hickman continue to develop new and effective techniques for pain control, like blocking the Distal Superficial Femoral Nerve Branches, which innervate the anterior distal thigh and knee. It’s a simple injection just superficial to the sartorius muscle and has essentially replaced the superior lateral genicular nerve block in Dr. Hickman’s practice.
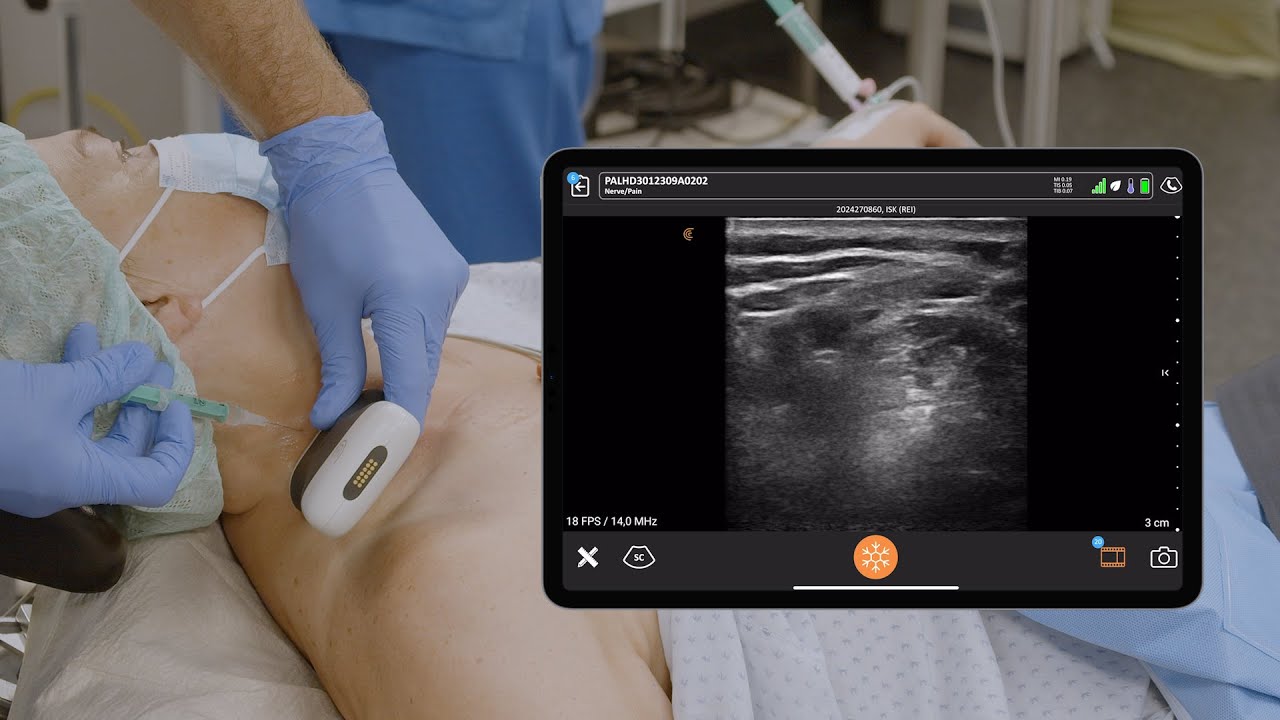
Handheld Ultrasound for Pain Management Procedures
High-definition imaging of musculoskeletal anatomy is now easy and affordable with handheld ultrasound, which provides image quality that is comparable to traditional cart-based ultrasound systems. To learn more about the high-frequency Clarius L15 HD3 handheld ultrasound scanner Dr. Hickman uses, contact us today or request an ultrasound demo.
To learn more about the difference ultra-high-definition imaging makes for regional anesthesia, visit our Anesthesia Specialty Page where you can access additional on-demand webinars, user reviews, and Classroom Videos.











{kind=link}