






By James Ferrie, B.Pod, M.A. Pod.A
A sought-after Podiatrist based in Melbourne, Australia, James Ferrie first started using ultrasound in his practice to guide regenerative injection therapy. Now he says it has become an invaluable tool for diagnostic purposes as well. Read his article to learn more.
As a Podiatrist, I’m very interested in the biomechanics and function of the foot. Unlike modalities like MRI, ultrasound lets me visualize anatomy dynamically and provides answers to clinical questions fast. Being able to ultrasound a patient on the spot helps improve the accuracy of my diagnosis and start treatment without delay. It saves my patients time, and it’s usually more cost-effective. It builds a patient’s trust and your confidence when you can point out pathology during the exam. The integration of a clinician’s detailed history and physical examination before an ultrasound scan is also extremely valuable.
Ultrasound imaging can be most valuable when in the hands of the clinician.
At times, there can be a disconnect between the treating doctor and the local radiology department. There can also be variability in terms of a sonographer’s skill set and interests. In many circumstances, the radiologist is reporting remotely and may not have sufficient information to integrate the patient’s history with the radiological findings.
Case study #1 – an unremarkable X-ray.
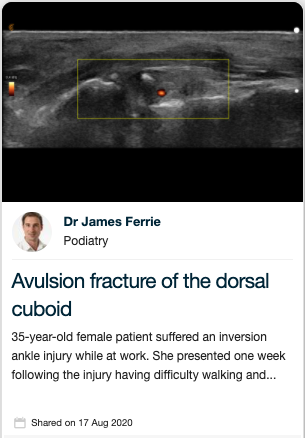
I recently had a patient who suffered from a workplace injury. The 35-year-old female patient fell at work, rolling her ankle. She reported feeling nauseous due to the pain and had difficulty weight-bearing after the injury. She immediately saw her General Practitioner (GP), who organized an X-ray and ultrasound. The X-ray was unremarkable, while the ultrasound revealed there was a grade one sprain to one of the ankle ligaments.
Ten days following the injury, her chiropractor referred her to me for a second opinion. She still had a lot of swelling and had trouble walking. There was extensive swelling, bruising and pain with palpation overlying the calcaneocuboid joint. Her history and physical exam were not consistent with the radiological report.
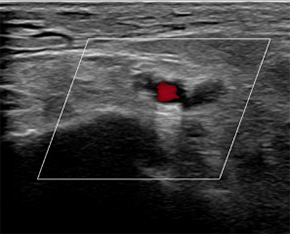
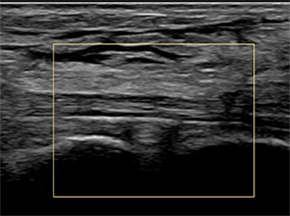
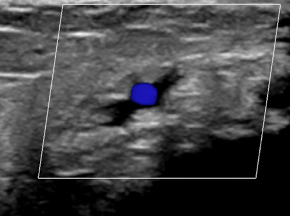
I scanned her with my Clarius L15 HD. The ultrasound scan revealed two boney fragments arising from the calcaneocuboid joint, with soft tissue oedema and hyperaemia of the periosteum seen with power Doppler. The clinical ultrasound findings were consistent with an avulsion fracture of the superior dorsal cuboid associated with bifurcate ligament injury, later confirmed on MRI.
Ultrasound lets me get quick answers to specific clinical questions to support the right course of treatment for my patients.
As clinicians, we listen and take a comprehensive history. Before physically assessing the patient, we have already comprised a provisional diagnosis and several differential diagnoses. The integration of point-of-care diagnostic ultrasound during a clinical examination adds a sixth sense, the ability to see below the skin, it helps to confirm or disconfirm my provisional diagnosis quickly and accurately.
Case study #2 – unexplainable ankle pain.
While working in a rural private practice, I had a healthy 35-year-old woman present with an acute onset of unilateral swelling medial ankle pain. She was limping as she walked into the consultation room. She reported the pain and swelling come on suddenly five days earlier; she could not recall any incident or injury. The pain had been unresponsive to ibuprofen.
On examination, there was generalized tenderness on palpation of the medial ankle with extensive soft tissue oedema.
In performing an ultrasound scan, there was extensive soft tissue oedema; however, I was unable to find a musculoskeletal cause for her presentation. I then continued scanning the tarsal tunnel and up the leg where I located a deep vein thrombosis in the tibial vein.
I referred her to the Emergency Department at the local hospital. She was assessed and advised it was likely a musculoskeletal injury, as she lacked the typical risk factors for DVT. They planned to discharge her with a script for some anti-inflammatories. Given clinical ultrasound, her husband insisted on a formal ultrasound, which confirmed a DVT in the tibial vein.
It turned out she had a clotting disorder, Factor 5 Leiden.
Ultrasound gives a clinician the confidence to put the patient first, allowing clinicians to, in many cases, confirm or disconfirm provisional diagnosis on the spot.
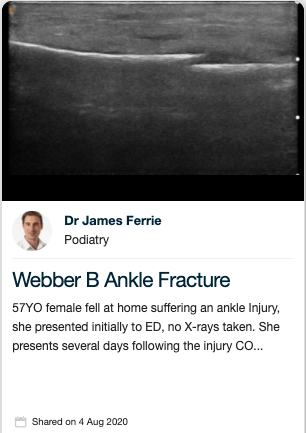
Case study #3 – not an ankle sprain.
A 57- year-old female tripped at home, suffering an ankle injury. She presented initially to the Emergency Department. She was discharged with a diagnosis of an “ankle sprain” without X-rays taken. She attended my clinic several days after, complaining of persistent pain and difficulty walking.
There was extensive oedema and focal pain on palpation of the distal fibula. Within several seconds of placing the Clarius L15 HD over the fibula, I could see the fracture. The long axis view demonstrates discontinuation of the cortex of the fibula with an effusive dome. X-rays confirmed the Webber B fracture.
Handheld scanners make it possible and affordable for every podiatrist to use ultrasound imaging.
With access to handheld ultrasound like Clarius, you don’t have to spend $20,000 – $30,000 on a complicated laptop system with buttons and knobs.
I’ve been using the Clarius L15 ultrasound scanner almost exclusively since it was introduced in Australia in April 2020. Its image quality is comparable to my laptop device, and overall, the L15 is better in many respects. From a medical-legal point of view, the reporting capability on the Clarius Cloud portal is fantastic, and one of the Clarius system’s big advantages.
I’m able to produce professional reports with my ultrasound findings to send to referrers, and as a result, I see more musculoskeletal referrals.
Clarius is also helpful with my training activities. I’m able to upload and save images securely on the cloud platform so I can easily share interesting cases with groups of podiatry colleagues who are new to ultrasound. I also use Clarius Live telemedicine to provide coaching sessions.
Billing for ultrasound can quickly offset the cost of a system.
My sonography skills integrated with clinical experience is crucial when making challenging diagnoses. I always give my patients the option to examine them immediately for a fee or to refer them. I find that 95% of patients will choose to have it done in my office, so I do hundreds of billable scans and ultrasound-guided interventions each year.
I started using ultrasound in my practice about five years ago when I was working in a rural location, with poor access to MSK imaging. I became interested in using ultrasound to guide regenerative medicine injection therapy. Now, I use ultrasound daily for enhanced diagnosis, and it has helped me provide better targeted patient care.
I still refer for certain things: for example, thoroughly scanning the forefoot can be complicated and time-consuming. Sometimes it’s also essential from a medical-legal point of view to have a second opinion on a complicated case. I refer to an excellent radiology department. I know the sonographers and the radiologists are very good at what they do. It’s not uncommon for them to find multiple issues.
As clinicians, we need to add the clinical context to pinpoint the problem that is causing the primary clinical concern and decide how to treat that effectively. That’s where I find my Clarius L15 HD helps visualize and sono-palpate the areas highlighted.
Proficiency with ultrasound builds confidence and trust, while dynamic imaging helps with difficult cases.
Utilizing my sonography skills, I’ve been able to set up a diagnostic and intervention clinic with a prominent Foot and Ankle Surgeon. We work with patients who typically have complex cases. Our goal is to pinpoint what precisely is causing the clinical problem to target intervention and surgical planning.
Our clinical sonographic findings help better understand the patient condition and guide conservative and surgical treatment planning. This level of insight can provide any clinician with vital information to better inform our patients.
James Ferrie uses the Clarius L15 HD handheld scanner. He is based in Melbourne, Australia and practices at two clinics: My Sports Podiatrist and Ultrasound Training Australia. Thank you James for sharing your success story! We enjoyed learning how ultrasound helped deliver better care in the three patient cases you shared with us.
To learn more about how easy and affordable it is to add Clarius HD to your podiatry or MSK practice, contact us today or request an ultrasound demo. We are happy to help!












{kind=link}