

During a recent webinar on ultrasound-guided pain procedures, renowned pain management expert Dr. David Rosenblum shared practical remedies for treating chronic pain. Focusing on a specific case, Dr. Rosenblum provided step-by-step instructions on how he performs an erector spinae nerve block using ultrasound guidance.
To hone your skills, read on for Dr. Rosenblum’s detailed tips and watch his Clarius Classroom video tutorial of an erector spinae block performed in clinic with one of his patients.
Case Study: Treating a 62-year-old Male Patient with Six Weeks of Pain in the Upper Back
“The patient had no past medical surgical history. His pain was localized deep to the rhomboid muscles. He felt some radiation laterally and anteriorly along the ribs. He had trigger points in the bilateral paraspinal regions. To alleviate his pain, I performed an erector spinae plane block.
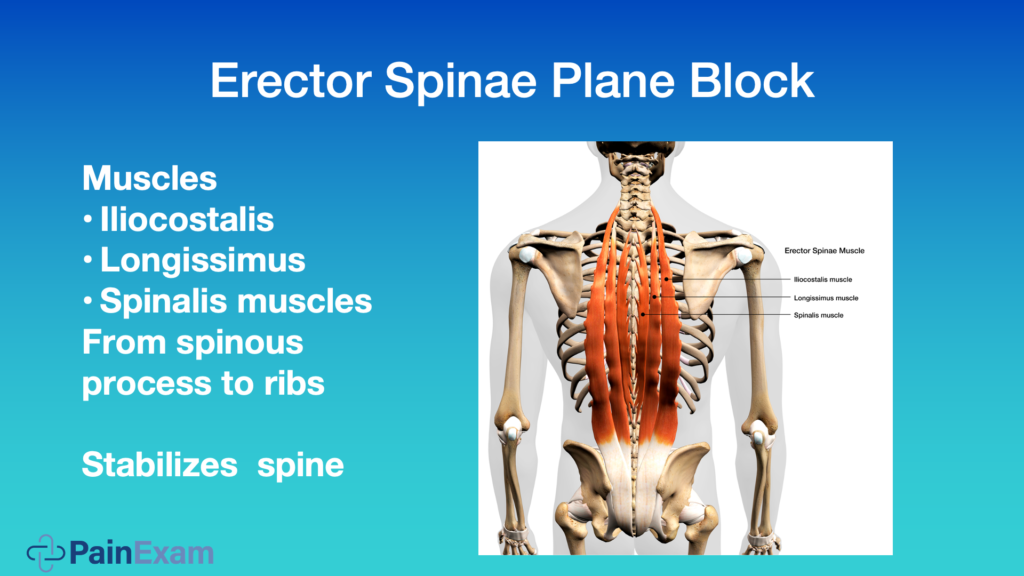
As you see depicted in this image above, the erector spinae plane is underneath the three muscles that form the erector spinae: the intercostalis muscle, the longissimus muscle and the spinalis muscle. They come from the spinous process to the ribs and they stabilize the spine.
You can see they run up and down the whole spine. So, you can do these blocks in a thoracic level or lumbar level.
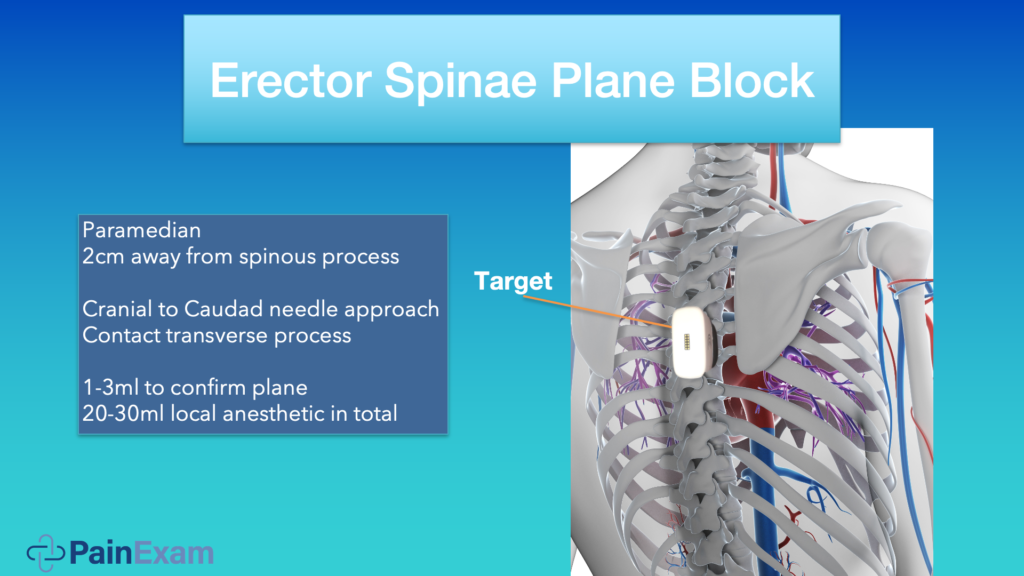
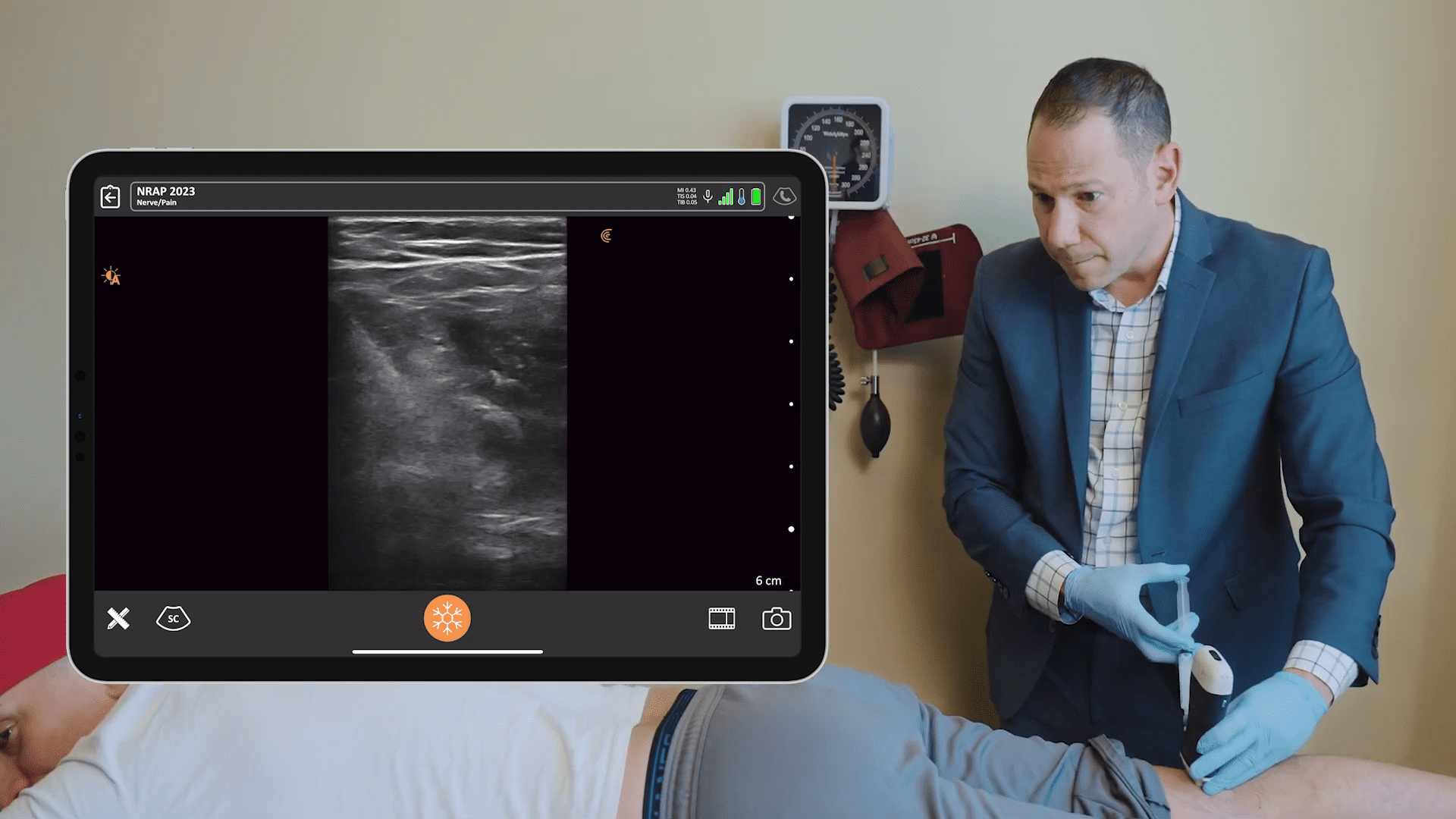
The erector spinae plane is typically two centimeters away from the spinous process. You can use cranial to caudad or caudad to crania needle approach. It really depends on the patient and what you’re doing. You want to contact the transverse process and then inject one or two MLs to hydrodissect, confirm you’re in the right plane, and inject the rest of the medication. On this image above, you see how I would position my ultrasound probe for this procedure.
Note: if you’re in the hospital for an anesthetic for surgery, you might use 20 or 30 MLs to get good spread and good coverage. If you’re in a pain office, you’re going to use a lot less and more diluted medication because a surgical level of anesthesia is not required.
A Review of the Anatomy for the Block
The Erector Spinae Plane nerve block is a less risky procedure than a paravertebral block, so it’s a great block if you’re not very experienced with blocks.
There are a few different theories on the mechanism of action. One is anterior diffusion of the local anesthetic into the paravertebral space, which makes sense. Or, interfacial spread towards the posterior rami of the spinal nerves, and this could help quite a bit with any musculoskeletal pain as well.
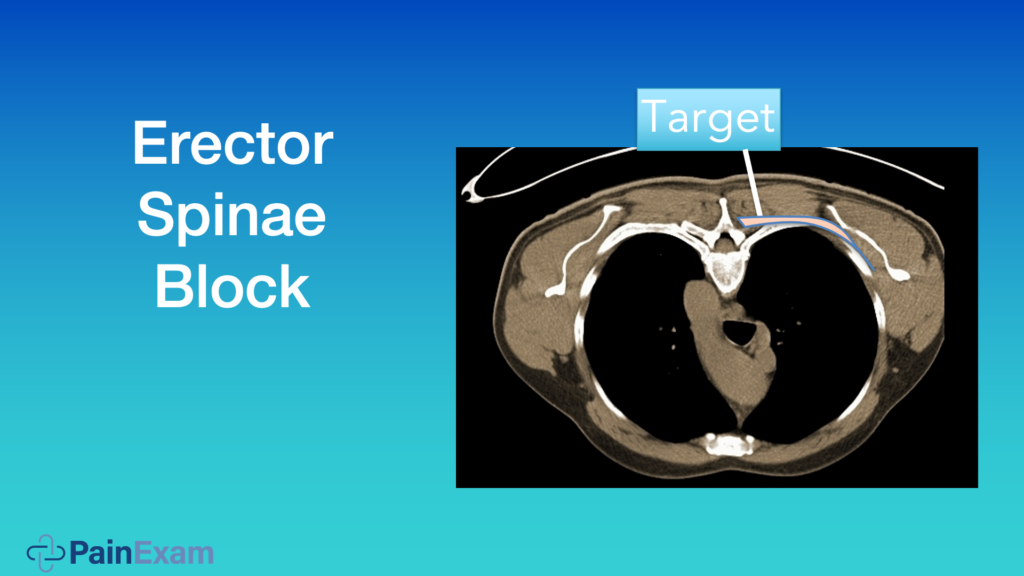
The image above shows you an axial cut of the thoracic spine, and you see the transverse process right before the ribs, or more lateral and underneath these muscles. This is the region you’re targeting, and the area highlighted in pink in the image below shows how the medication spreads. Some may go a little bit anterior to the paravertebral space as well, which is not shown here.
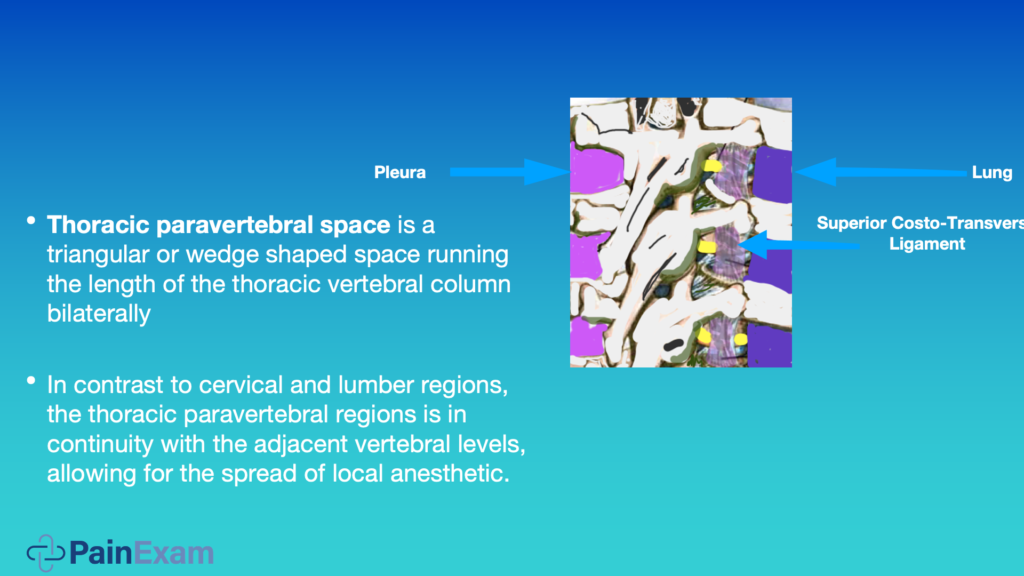
Paravertebral nerve blocks are extremely useful. Basically, the anatomy is a wedge-shaped column running up and down the thoracic spine. Unlike the lumbar and cervical levels, this area is continuous, meaning when you give a T4 paravertebral nerve block, you’ll get spread to T2, to T6; it really depends on how much volume you give. It’s like an epidural. You’re filling up a column.

For patients who have multiple rib fractures, you could just do one paravertebral nerve block and even place a catheter and it helps. When you get into the paravertebral space, you may have a loss of resistance. Of course, aspirate for blood, CSF, or even air. Hopefully you don’t get any of those. And then you want to inject.

Above is a view of our block using sonar vision. The star on this video is our target for the paravertebral nerve block. This video was captured with my Clarius L7 HD. You can see the lung moving. You see the pleura moving. The triangular shaped space is the paravertebral space.
You can see the thoracic transverse process, which, if you scan high or low, you could get out of the screen. You’ll see my needle coming on in from lateral to medial. And the target’s over here. The pleura, lamina and spinous process are labelled to give you some perspective.
I’m using a 25-gauge 3.5” needle. It’s harder to see but I use it because it’s less painful for the patient. I can see it and am very comfortable with it. You’re going to see a lot better if you use an echogenic needle. The target for the ESP block is on the transverse process.
Video Case Study Demonstration: Erector Spinae Block
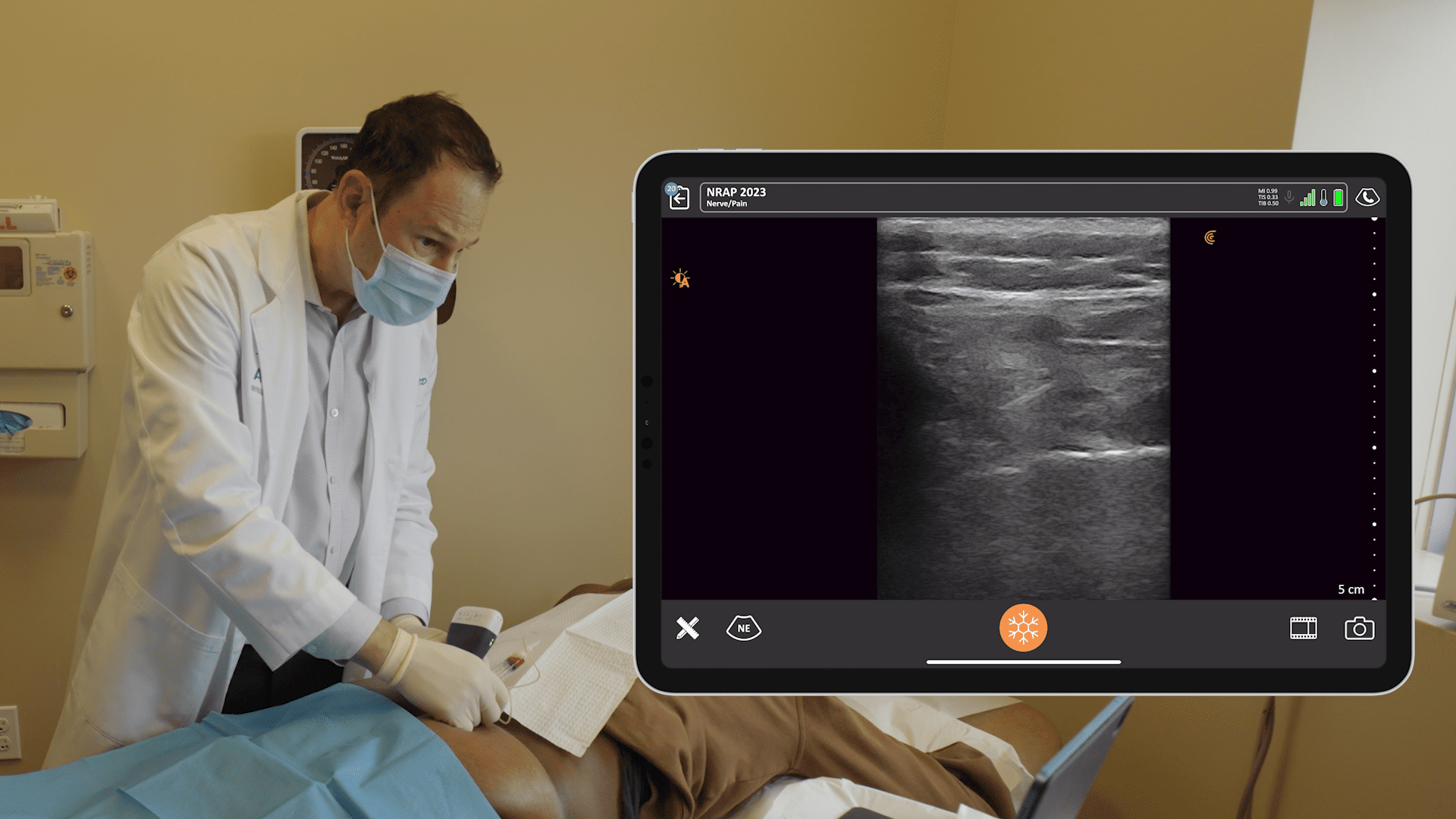
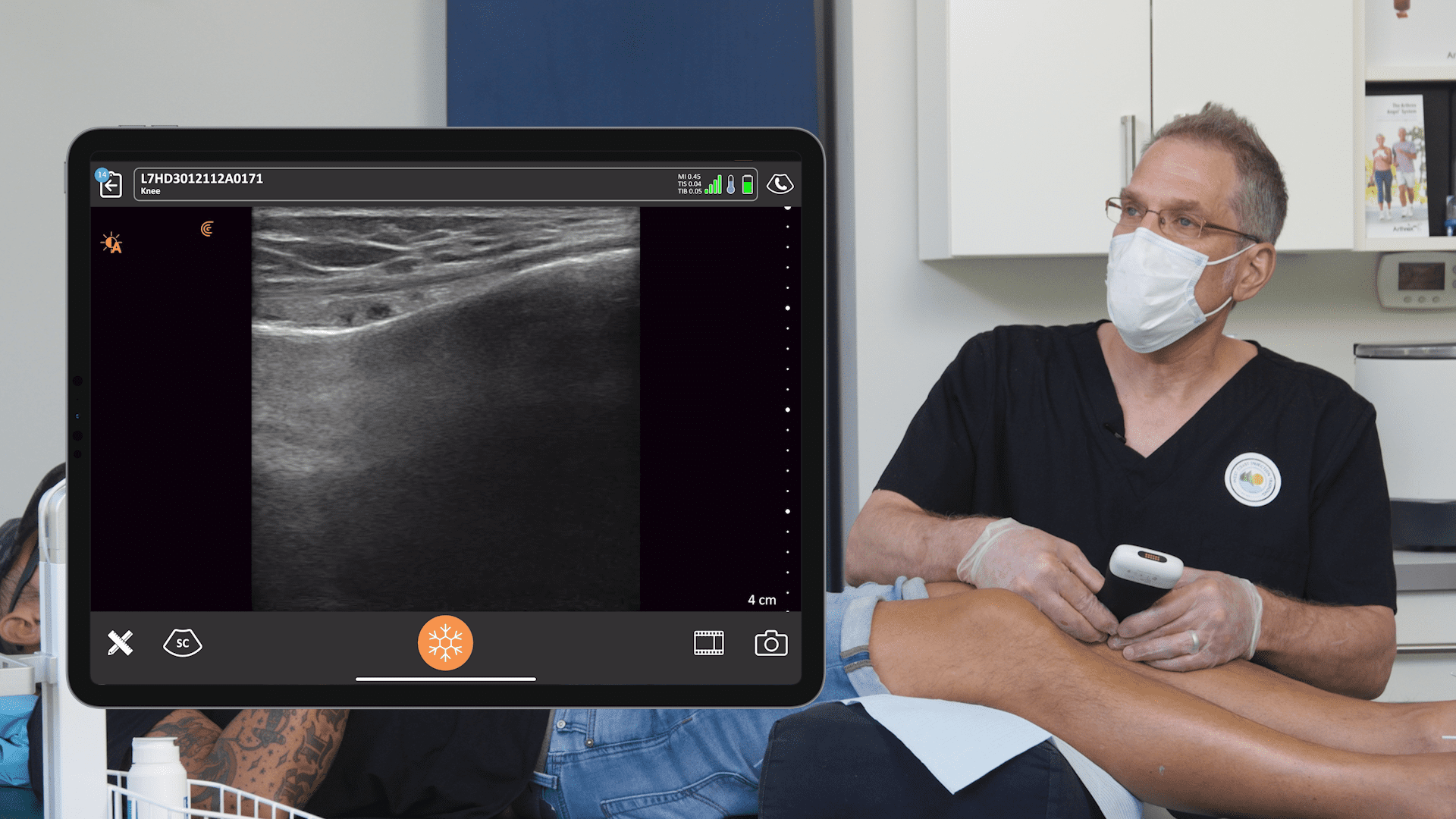
Watch the following video to see the block captured in real-time in my office. The patient had pain in the lower back. What we did was trigger points of his lower back. I also anesthetized the erector spinae muscle and got into the plane to help alleviate some of his pain. He does have some pain radiating down, and I let some of the local anesthetic go into the intercostal space as well to help him with the pain that’s referred from the paravertebral space on the left side in the lower ribs down to his flank.
In the video, I’m using the Clarius L7 HD Linear scanner, which is a mid-frequency range probe. I use it to look at the spinous process, the lamina, and the transverse process in lateral. You see the transverse process and the superior articular process. I give the patient a little bit of a vapo-coolant spray prior to inserting the 25-gauge needle. The patient is slim.
Besides back pain, the Erector Spinae Nerve block is useful for a lot of different things including acute care for renal colic, rib fractures, putting in chest tubes, shingles pain on the thorax, anything that ails you basically.”
Watch the Webinar to Learn More Practical Pandemic Pain Remedies
If you’d like to learn more practical tips from Dr. Rosenblum, watch the full webinar at your convenience. Or watch two more of his new Clarius Classroom video tutorials on how to use ultrasound guidance to safely perform an occipital nerve block and a gluteal tendon injection.
Dr. Rosenblum is the Director of Pain Management at the Maimonides Medical Center in New York. A prolific educator, he hosts the Pain Exam Podcast and created a Pain Exam Board Review, which has helped more than 3,000 pain management physicians become board certified. Dr. Rosenblum’s program Private Ultrasound Instruction for Regional Anesthesia & Pain Management is available now on his Pain Exam website.
To learn more about how Clarius HD is used to guide injections, visit our wireless ultrasound for pain management page. Or contact us to today to book a demo with one of our ultrasound experts.








{kind=link}